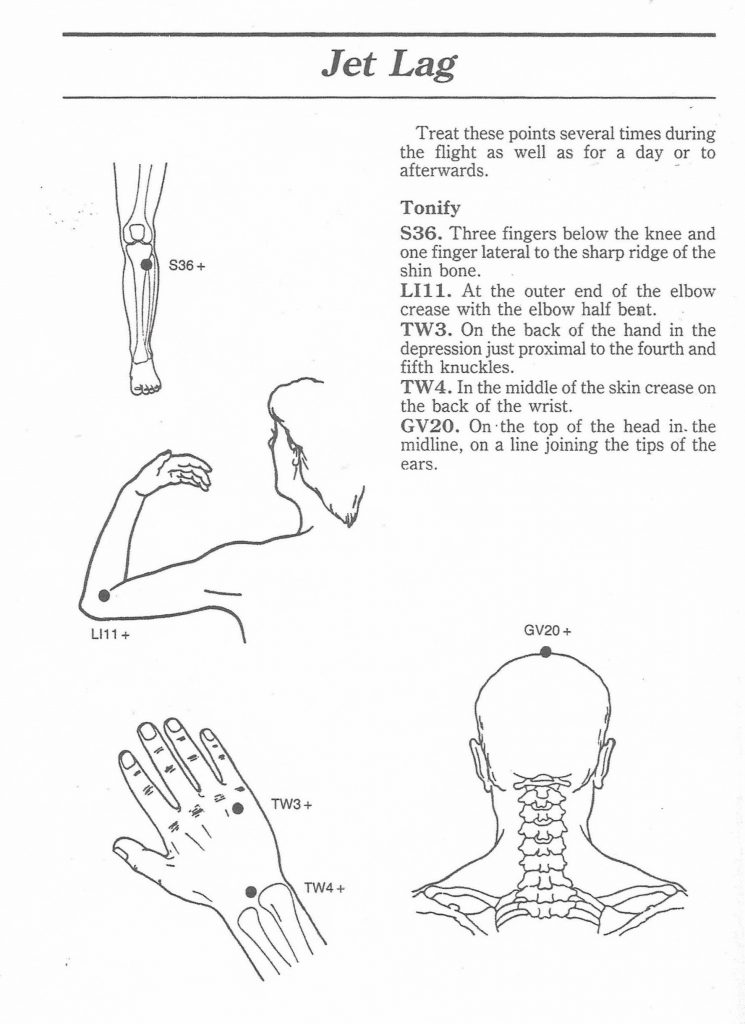
JET LAG 2 Additional points
See the bottom of this article for two more concerning diet and health including one about breast cancer.
Natural Medicine Journal
Published on Natural Medicine Journal (https://www.naturalmedicinejournal.com)
November 2019 Vol. 11 Issue 11
Skipping Breakfast Associated with Increased Cardiovascular Disease and Death
Results of a prospective cohort study
By Jacob Schor, ND, FABNO
Reference
Rong S, Snetselaar LG, Xu G, et al. Association of skipping breakfast with cardiovascular and all-cause mortality. J Am Coll Cardiol [1]. 2019;73(16):2025-2032.
Study Objective
The authors examined the association of skipping breakfast with cardiovascular and all-cause mortality.
Design
This is a prospective cohort study. Frequency of eating breakfast was compared to cardiovascular and all-cause mortality risk using weighted Cox proportional hazards regression models.
Participants
The study followed a cohort of 6,550 US adults, 40 to 75 years of age, who participated in the National Health and Nutrition Examination Survey III 1988 to 1994. Frequency of breakfast eating was recorded during an in-house interview. Death and underlying causes of death were ascertained by linkage to death records through December 31, 2011.
Key Findings
In following this cohort for 17 to 23 years, the researchers found that skipping breakfast was associated with a significantly increased risk of mortality from cardiovascular disease. Of the cohort, 59% consumed breakfast daily. The other 40% ate breakfast less frequently: 5% never ate breakfast, 11% rarely ate breakfast, and 25% ate only on some days. The study produced 112,148 person-years of follow up data, during which 2,318 deaths occurred, including 619 deaths from cardiovascular disease (CVD).
After adjustment for age, sex, race/ethnicity, socioeconomic status, dietary and lifestyle factors, body mass index, and cardiovascular risk factors, participants who never consumed breakfast compared with those who consumed breakfast everyday had hazard ratios of 1.87 (95% confidence interval [CI]: 1.14-3.04) for cardiovascular mortality and 1.19 (95% CI: 0.99-1.42) for all-cause mortality. The latter upward trend did not reach statistical significance.
After adjustment for age, sex, and race/ethnicity, participants who never consumed breakfast had a 75% higher risk of all-cause mortality (hazard ratio [HR]: 1.75; 95% CI: 1.46-2.10) and 2.58-fold higher risk of cardiovascular mortality (HR: 2.58; 95% CI: 1.64-4.06) compared with those who consumed breakfast every day. The associations of breakfast eating with heart disease–specific and stroke-specific mortality were examined further. Compared with those who consumed breakfast every day, participants who never consumed breakfast had a higher risk of heart disease–specific mortality (HR: 2.34; 95% CI: 1.44-3.80) and stroke-specific mortality (HR: 3.53; 95% CI: 1.40-8.95) in models adjusted for age, sex, race/ethnicity. In the fully-adjusted model, the association between skipping breakfast and stroke-specific mortality remained significant (HR: 3.39; 95% CI: 1.40-8.24).
Practice Implications
According to this study eating breakfast regularly reduces risk of dying from cardiovascular disease and probably stroke. Or, put another way, not eating breakfast raises risk significantly. We should foster in our patients the habit of eating breakfast.
Keep in mind that more people die of cardiovascular disease than any other cause—not just in the United States but worldwide. Even small decreases in risk have the potential of having large impacts on disease and suffering.
We often hear that “breakfast is the most important meal of the day.” I had always assumed this was merely an advertising slogan invented by Kellogg’s to sell their breakfast cereals a century ago. Surveys tell us that almost a quarter of younger people skip breakfast daily. It looks as though this may have long-term detrimental effects on their health.
Accumulating evidence, while limited, suggests that skipping breakfast is associated with increased risk of overweight/obesity, dyslipidemia, hypertension, type 2 diabetes, metabolic syndrome, coronary heart disease, and cerebrovascular disease.
It’s not just about eating breakfast. Skipping breakfast may also signal other unhealthy dietary and lifestyle habits. Teenagers who skip breakfast tend to exhibit a list of other traits that may also put their health at risk (eg, eating more fast food, having more emotional problems). Asking patients if they eat breakfast is similar in a way to the old patient intakes in which we asked patients if they used seatbelts. A negative response may hint to a pattern of unhealthy lifestyle choices.
This is not the first study to suggest a negative association with skipped breakfasts. Cahill et al reported in 2013 that they had assessed the eating habits of 26,902 American men from the Health Professionals Follow-up Study. During a 16-year period, 1,527 cases of heart disease were diagnosed among these men. Men who skipped breakfast had a 27% higher risk of coronary heart disease (CHD) compared with men who did not (relative risk (RR): 1.27; 95% CI: 1.06-1.53). Furthermore, we should note that men who ate late at night had a 55% higher CHD risk compared with men who did not eat late at night (RR: 1.55; 95% CI: 1.05-2.29).9
Kubota et al reported results in a 2016 paper from a large group that included 82,772 participants (38,676 men and 44,096 women) in Japan. Those people who skipped breakfast had a 14% greater risk of CVD, an 18% increased risk of stroke, and a 36% greater risk of hemorrhagic stroke.10
The discussion now is not if skipping breakfast is bad by why. Several theories have been postulated. Skipping breakfast might lead to overeating later in the day and impaired insulin sensitivity. Eating breakfast helps regulate the appetite and improves the glycemic response at the next meal, increasing insulin sensitivity. Skipping breakfast is stressful, and the longer period of fasting leads to elevated blood pressure in the morning because of a hypothalamic-pituitary adrenal triggered response.
Eating breakfast on the other hand lowers blood pressure and reduces arterial stiffness. This is why measurements of these parameters are done in a fasting state. Skipping breakfast may also trigger unwanted changes in blood lipids, in particular increased LDL cholesterol.5
Whatever the reasons, data consistently shows skipping breakfast increases risk of cardiovascular disease. The advice to have breakfast may meet with resistance among those who fast overnight for their health.
Carol Marinac, in a 2016 paper noted the association of longer night-time fasting and lower risk of breast cancer recurrence. Specifically, the data showed that those who fasted more than 13 hours had less breast cancer recurrence. We covered this study [2] in 2016.
The problem with encouraging this type of fasting is that many people fulfill the 13-hour fasting suggestion by simply skipping breakfast. The resultant increase in CVD risk might outweigh any breast cancer risk reduction. We need an approach that will allow both a longer night-time fast and encourage eating breakfast, so the obvious solution would be to eat an earlier dinner. Such a meal pattern of eating an early dinner was encouraged by Kogevinas et al’s 2018 study. In those results, compared to participants who went to sleep immediately or shortly after supper, those who delayed going to sleep for 2 or more hours after supper had a 20% reduction in risk for breast and prostate cancer combined (adjusted odds ratio [OR]: 0.80; 95% CI: 0.67-0.96) and in each cancer individually (prostate cancer OR: 0.74; 95% CI: 0.55-0.99 and breast cancer OR: 0.84; 95% CI: 0.67-1.06).16 Read our coverage [3] of that study.
If we combine Kogevinas’s findings with Marianac’s, then we should encourage an early dinner (minimum of 2 hours before bedtime) and then breakfast 13 hours later. Once again, the research suggests that when we eat may deserve as much attention as what we eat.
About the Author
Jacob Schor ND, FABNO, is a graduate of National College of Naturopathic Medicine, Portland, Oregon, and recently retired from his practice in Denver, Colorado. He served as president to the Colorado Association of Naturopathic Physicians [6] and is on the board of directors of the Oncology Association of Naturopathic Physicians [7]. He is recognized as a fellow by the American Board of Naturopathic Oncology. He serves on the editorial board for the International Journal of Naturopathic Medicine, Naturopathic Doctor News and Review (NDNR), and Integrative Medicine: A Clinician’s Journal. In 2008, he was awarded the Vis Award by the American Association of Naturopathic Physicians. His writing appears regularly in NDNR, the Townsend Letter, and Natural Medicine Journal, where he is the Abstracts & Commentary editor.
References
PROTEINS
Here’s What Actually Happens in Your Body When You Eat Protein
Besides help you make those #gains at the gym, of course.
Self.com
While carbs and fat get alternately praised and punished, protein is basically the golden child among the macronutrients. That’s totally unfair to carbs and fat, first of all, but protein certainly does enough to earn its reliably good reputation. We know protein is a great thing to have, but why exactly do we need it, and what does our body even do with it? Here’s a rundown of what actually happens when you eat protein.
What protein actually is
Like we mentioned, protein is one of the three macronutrients (i.e. nutrients the body needs in sizable amounts). Unlike carbs and fat, protein is not usually a major energy source, although we definitely get some of that from it—protein provides 4 calories per gram. But protein is often referred to as a building block in the body because of its central role in growth and development.
Almost all animal-derived products—meat, poultry, eggs, dairy, fish—contain a significant amount of protein, so they get labeled as “proteins” when we’re talking about our diets and nutrition. But protein is also present in a lot of plant-based foods. There’s a good amount in beans, peas, nuts, and seeds, for instance, while vegetables and grains generally contain smaller amounts, according to the FDA. (Whole grains will have more protein than refined grains, though, which are missing the part of the grain that often supplies a lot of the protein content, as SELF previously reported.)
The different kinds of proteins
Proteins are made of small units called amino acids. Amino acids are organic compounds containing structures made of elements including nitrogen, hydrogen, carbon, and oxygen. Hundreds or thousands of amino acids link up to form super long chains, and the sequence of that chain determines the protein’s unique function, the U.S. National Library of Medicine explains.
There are 20 different amino acids in total, which can be broken down into two main groups, per the FDA. Nine of the 20 are what are referred to as essential amino acids, meaning that the body is unable to produce them itself and so we must get them from food. The other 11 are nonessential because the body is able to synthesize them out of the essential amino acids or the normal process of breaking down proteins, according to the U.S. National Library of Medicine. Many of these nonessential amino acids are also considered conditional amino acids, because they can become essential in rare, severe instances when the body is unable to synthesize amino acids properly, per the U.S. National Library of Medicine.
Now, when a protein is a good source of all nine of the essential amino acids, we call it a complete protein, according to the FDA. All animal products are complete proteins, and so is soy. When a protein is missing or pretty low in any of those essential amino acids, it’s considered incomplete. Most plant foods are considered incomplete proteins.
The good news for vegetarians, vegans, and lovers of plant foods in general is that you can still easily get all the essential amino acids from eating a wide variety of incomplete proteins. As the FDA explains, incomplete proteins are often just lacking in one or two amino acids, so they can often make up for whatever the other one is lacking. (Pretty romantic, right?) For instance, grains are low in an amino acid called lysine, while beans and nuts are low in methionine. But when you eat, say, beans and rice or wheat toast with nut butter, you’re getting all the amino acids that you do when you eat, say, chicken. While people used to be encouraged to eat foods in combinations at meals, we now know this is not necessary, according to the U.S. National Library of Medicine, as long as you’re eating a variety of complementary incomplete proteins throughout the day.
Why we even need protein
That building block nomer is no exaggeration. The stuff is an integral component of every cell in the body, including, yes, your muscles. “If we don’t get enough protein, our bodies actually won’t be able to rebuild properly and we’ll start to lose muscle mass,” Colleen Tewksbury, Ph.D., M.P.H., R.D., senior research investigator and bariatric program manager at Penn Medicine and president-elect of the Pennsylvania Academy of Nutrition and Dietetics, tells SELF.
In addition to muscle growth, protein is essential to the growth and repair of virtually all cells and body tissues—from your skin, hair, and nails to your bones, organs, and bodily fluids, according to the FDA. That’s why it’s especially important to get enough of it during developmental periods like childhood and adolescence.
Protein also plays a role in crucial bodily functions like blood clotting, immune system response, vision, fluid balance, and the production of various enzymes and hormones, per the FDA. And because it contains calories, it can provide the body energy for storage or use. (But this definitely isn’t its main gig, which we’ll get into in a bit.)
What happens in your body when you eat protein
It’s not like we eat a piece of chicken and that protein goes directly to our biceps. Dietary protein gets broken down and reassembled into the various kinds of proteins that exist in the body. No matter what kind of protein you’re eating—plant or animal, complete or incomplete—the body’s first objective is to break it back down into all the different amino acid units it was assembled from, Tewksbury explains.
Breaking down protein requires more time and effort than carbs, but not as much as fat. It begins in the mouth, as proteins and especially animal proteins typically take more chewing than other kinds of foods, Tewksbury says. That mechanical process is the very first step of digestion.
Then, those pieces of protein move to the stomach to get mixed up with gastric juices containing acids and enzymes that help break down food. Next, that mixture gets passed on in steady increments to the small intestine, where more specialized enzymes and acids get injected (mainly by the pancreas) to help break that protein all the way down. Once you’ve got those little singular amino acids, they’re ready to get to work.
How the body uses protein
These amino acids get sent to the liver, where they’re shuffled around and reconfigured into any type of protein your body needs, Tewksbury explains. Your body is constantly regenerating and replacing cells and tissues, so there’s always a variety of proteins needed. For instance, some proteins in the body make up antibodies that help the immune system kick out bacteria and viruses. Others help with DNA synthesis, chemical reactions, or transporting other molecules, the National Institute of General Medical Sciences explains.
How much protein your body actually requires for the purpose of tissue growth and repair is determined by factors like sex, age, body composition, health, and activity level, according to the U.S. National Library of Medicine, but most of us are getting more than enough protein to fulfill these needs. The bummer is that once your tissues get all the amino acids that they need, they have no use for any extra.
So what happens to the rest, once our dietary protein intake exceeds what our tissues need? The body doesn’t have a protein holding tank like it does for carbs, where it can siphon away extras for quick access when we need it. “We have little to no way of being able to store protein [for future use] in our body,” Tewksbury explains. This is why you need to eat protein throughout the day, every day.
Since we can’t use excess protein for its intended purpose later on, the body breaks it down and stows it away in fat tissue, according to Merck Manuals. To do this, the liver removes the nitrogen from the amino acids and disposes of it through the urine, in the form of a waste product called urea, Linsenmeyer explains. What’s left behind is something called alpha keto-acids, which will most often then go through a chemical process that turns them into triglycerides to be stored in our fatty tissues, Linsenmeyer says. (This can technically be accessed at a later date when the body needs to tap into fat stores for energy.)
Alpha-keto acids can be converted into glucose and used for immediate fuel if necessary, when the body is in a fasting state or not getting enough calories coming in from other macronutrients, Linsenmeyer says. But this is not typical because the body prefers carbs as its primary source of energy, followed by dietary fat, which the body can adapt to use as fuel if it’s not getting enough carbs. “We can adapt to use protein for energy as well, but it’s not ideal,” Linsenmeyer says. “Ideally, [our bodies] want to leave it alone to build and maintain body tissues.”
Now, what we just walked you through is still oversimplifying the reality of what happens when we eat protein (or any food). Digestion and metabolism are complex processes happening constantly on a cellular level. But even just grasping the broad strokes can make you really appreciate what your body actually does with the protein you eat.
LOST SENSES
SMELL
Here is an article about a woman’s journey after losing her sense of smell.
Here is a site to help you hopefully regain your sense of smell
HEARING
Here is an article about low levels of a hormone Aldosterone can cause reduced hearing acuity.
I posted about Aldosterone previously on my web site. Just do a search
Systemic enzyme therapy is the use of oral proteolytic enzymes such as trypsin, chymotrypsin, papain, and bromelain taken on an empty stomach. Since stomach acid can destroy proteolytic enzymes, the best formulas are “enteric coated” tablets or “delayed release” capsules. Enteric-coating means that the pills have a coating around them to prevent the pill from being broken down in the stomach. “Delayed release” vegetarian capsules use natural dietary fibers that also resist stomach acid to provide targeted delivery of the enzymes to the upper small intestine. Clinical research, anecdotal evidence, and a long history of use has shown that proteolytic enzymes can systemically support circulation, healthy inflammatory response, and recovery of the musculoskeletal system after overexertion.*
Several studies have shown that proteolytic enzymes can help support muscle recovery after exercise.* A 2009 study published in the Journal of International Society of Sports Nutrition demonstrated efficacy with a product that contained proteolytic enzymes combined with curcumin.* A 2004 study published in the Journal of Sports Science demonstrated that proteolytic enzymes reduced muscle soreness after downhill running.*
Several randomized, double-blind, placebo-controlled trials have shown that systemic enzyme therapy can help support healthy joint function.* This includes a 2015 study published in the journal Arthritis, a 2004 review of clinical studies published in Evidence-based Complementary and Alternative Medicine, and a 2004 trial published in Clinical Rheumatology.
A 2018 randomized double-blind controlled trial published in the Journal of Phlebology and Lymphology using systemic enzymes in people needing extra vein support demonstrated that the supplemental enzymes were “safe and effective.”
When proteolytic enzymes are given on an empty stomach, they can systemically support the musculoskeletal system on many levels.* There are several high-quality systemic enzyme supplements presently available for integrative practitioners to choose from for specific musculoskeletal applications.
Boswellia serrata (Boswellia), also known as Indian Frankincense, is a moderate-sized tree native to India, Northern Africa and the Middle East. Boswellia is an herb that is commonly used in Ayurveda. Resins from Boswellia trees have been used since ancient times to support joints as well as other health concerns. The boswellic acids from the resin of the trees have been shown to specifically support a healthy inflammatory response in joints following exercise or occasional overexertion.* Research has confirmed that Boswellia can suppress leukotriene synthesis by influencing the 5-lipoxygenase pathway, which helps support healthy cartilage.*
A 2018 review published in the Indian Journal of Pain concluded that a product containing Boswellia helped support cartilage structure and joint function.* This is consistent with a 2013 randomized, double-blind, controlled trial involving 440 study participants that was published in the journal Rheumatology. In that 2013 trial, overall knee function was improved.* A 2016 review published in Advances in Pharmacological Sciences also showed that Boswellia supported joint function.* A 2018 review published in the Journal of Clinical Orthopaedics and Trauma featured Boswellia as one of the top 10 nutraceuticals used to support joint and cartilage health in India.* The researchers also confirm that no serious side effects have been reported with the use of Boswellia.
It’s clear that there is solid research showing the health benefits of this popular Ayurvedic herb. Boswellia is available as a dietary supplement as a single herb or in combination with other herbs that have been shown to support joints, cartilage and a healthy inflammatory response.*
| Top 8 Recommended Essential Oils For Respiratory Health + Tips on Using Essential Oils https://www.journalofnaturalmedicine.com/top-8-recommended-essential-oils-for-respiratory-health-tips-on-using-essential-oils/ Essential oils are one of the best options for restoring respiratory health. Essential oils can quickly and effectively reduce swelling in the respiratory tract, help expel phlegm, and improve breathing. Their effect can be felt almost instantaneously and there are little to no adverse side effects when using essential oils for respiratory health. There is quite a large variety of essential oils available for an even wider variety of ailments. Most essential oils are available at low price points, making them a great, inexpensive choice for addressing ailments. A little oil, just a few drops goes a long way, so even the pricer oils are still a great, natural, cost-effective option.1. Lemon Essential OilLemon oil is an effective essential oil when it comes to congestion and coughs. The oil is derived from the skin of lemons. It is useful for treating sore throats in association to its antioxidant, antibacterial, and antioxidant properties. Scientific research and evidence has shown that lemon oil is able to inhibit bacteria growth and improve the immune system. In the Journal of Antimicrobial Chemotherapy, a study was published in 2001, which stated that antibacterial actions of essential lemon oil was effective against allergy and cold symptoms.2. Frankincense Essential Oil Frankincense essential oil is regarded as a highly powerful oil. Years ago, frankincense was at a stage valued higher than gold. Today, this oil is a fantastic anti-inflammatory when it comes to clearing nasal passages and lungs along with the regulation of breathing patterns. More specifically, it can assist in expelling phlegm out of the lungs. When treating a cold or a cough, use 2 to 3 drops of the oils in a diffuser.3. Peppermint Essential Oil Studies have suggested that antispasmodic activities in peppermint essential oil can help relieve coughing. This oil is better known when it comes to its antibacterial, antiviral, anti-inflammatory, antispasmodic, expectorant and antimicrobial properties. Peppermint is commonly used to treat respiratory infections, sinus infections, colds, sore throats and coughs. In the Journal of Ethnopharmacology a study which was published in 2010 has suggested antispasmodic activities in essential peppermint oil assists in relieving coughs. Menthol present in this oil is believed to soothe and calm sore throats, while relieving a cough in the way of thinning mucus.4. Tea Tree Essential Oil This essential oil contains antiviral, antiseptic and antimicrobial properties. Tea tree is a fantastic oil when it comes to bronchial congestion. This oil has been discovered to exhibit exceptional protective activities against fungi, yeast, and bacteria, which can be found in a study which has was released in 2000 from a German research team. Microbes are what cause inflammation that can deplete the person’s immune system, which often results in congestion and coughs and susceptibility to other infections. Tea tree essential oils contain antiviral, antiseptic and antimicrobial properties that fight off these microbes. This essential oil is effective for bronchial congestion, coughs and sore throats. For relief, apply 15 drops of a good quality tea-tree oil to the sinuses and neck for an effective cough remedy.5. Eucalyptus Essential Oil Eucalyptus oil is proven to be a useful aid for treating upper-respiratory infections and congestion. This high-quality oil also loosens mucus and lowers respiratory inflammation inside the lungs. Eucalyptus is found in a variety of over-the-counter products when it comes to congestion, cough and cold relief. This is an essential oil associated with many health benefits when it comes to its effective abilities in improving respiratory circulation, stimulating the immune-system, and providing antioxidant protection. The active ingredient in this oil is known as cineole. With many long-term studies it has been indicated that essential eucalyptus oils are useful for treating upper-respiratory infections and congestion.6. Thyme Essential Oil Research suggests that thyme essential oil can assist in supporting the respiratory and immune systems. This is a preferred essential oil when it comes to congestion and coughs in association to its antimicrobial, antioxidant and antibacterial properties. It is these effects which assist in supporting the respiratory and immune systems. In 2011, there was a study which was published in the Medicinal Chemistry journal, where researchers studied the response of thyme oil to 120 different bacteria strains which were isolated from people suffering from respiratory infections. Results showed that this oil displayed strong activities against each of these bacteria strains. This means thyme essential oil is ideal for congestion, coughs and sore throats caused from colds and flu and other related illnesses.7. Juniper Berry Essential Oil This essential oil features over 87 active ingredients that includes antimicrobial, antifungal, antibacterial and antioxidant agents. Juniper Berry essential oil has a sweet and woodsy smell, which is found in various aromatherapy blends, fragrance sprays, and even household-cleaning products. This is an essential oil that is typically used for treating respiratory infections as well as sore throats. Research has gone onto show that this important essential oil has over 87 active ingredients which include antimicrobial, antibacterial, antioxidant and antifungal agents. In 2003 a study appeared in the Phytotherapy Research journal which discovered that antimicrobial activities associated with juniper oil was due to the combination of the compounds known as alpha-pinene, p-Cymene and beta-pinene.8. Clove Essential Oil Clove essential oil displays antimicrobial activities against various multi-resistant bacteria. This essential oil is commonly used for relieving sore throats, boosting the immune-system, which has to do with its stimulating, antiviral, antifungal, anti-inflammatory, antimicrobial and antiseptic properties. In the journal Phytotherapy Research a study was published in 2007 discovered that essential clove oil displays activities against several multi-resistant bacteria. When you feel a sore throat coming on or you are starting to cough, placing 1 drop of clove oil on your tongue is an effective remedy for these common issues. Tips On Using Essential Oils For Congestion, Colds and Cough1. Aromatherapy: Adding Essential Oils To DiffusersAromatherapy is an age old yet effective practice to relieve coughs. Add drops of your chosen essential oil into the diffuser. Diffusers are one of the best ways to use the above mentioned essential oils when it comes to coughs and congestion we described earlier on. A diffuser of high-quality is a worthwhile investment. These diffusers work on breaking the essential oil down into very small molecules that spread through the air. This process will improve air quality in the room that you use it in. In this way diffusers work well for treating flu, sinus infections, congestion and colds.2. A Hot And Healing Bath Soak One of the other effective ways to use essential oils for colds, congestion and coughing is to add the oil into hot water in a bath. Relaxing and soaking in hot water with your favorite essential oil can work wonders when fighting a cold or flu. Below is a recipe you may want to try:Ingredients– 6 Drops of Tea Tree Oil– 2 Drops of Thyme OilDirectionsAdd both the essential oils into hot or warm water in your bath. Make sure you do not use more than the recommended dose of thyme oil as it can result in irritation. You can also add some lavender or eucalyptus epsom salt to relax your muscles and joints. Relax and enjoy a healing bath. Four Powerful Health Benefits of Elderberry https://www.journalofnaturalmedicine.com/four-powerful-health-benefits-of-elderberry/ Elderberries contain a variety of potent health benefits. Many individuals have consumed this dark berry in juice, jams, wine, or other culinary preparations without being aware of the health benefits of elderberry. Known scientifically as Sambucus Nigra, this medicinal berry comes in many varieties, the most popular being the European elder and the American elderberry. Both of these varieties contain powerful health benefits. Elderberry is also referred to as sambucus— its botanical name. Elderberries do contain low levels of naturally-occurring cyanide so it’s important to source them from a reputable seller. What Is Elderberry?Elderberry is a genus of flowering plants. It grows in various varieties, the most popular being the European elder and the American elderberry. The elderberry tree is identifiable by its clusters of tiny, flat, white flowers and bundles of elderberries. Common names for elderberry are Elder, American Elder, Black Elderberry, Boor Tree, Common Elder, Ellhorn, European Elder, Holunder, Holunderbeeren, Sambucus, Sambuci, and Sureau. Both the American and European elderberry contain the anthocyanin and polyphonol-rich black berries from which jams, juice, syrups, and other foods are made from. The flesh of the berry is the only edible part of the plant; in fact, the seeds, stems, leaves and roots of the black elder contain a cyanide-inducing glycoside that is poisonous to humans. Cooking the elderberries eliminates the glycosides present in the seeds, making them safe to eat. Additionally, exposing the berries to heat concentrates the anthrocyanins and polyphenols.Health Benefits of Elderberry1. Elderberries are rich in various beneficial compounds including: Anthrocyanins– Anthrocyanins are a subgroup of the flavonoid class. Research has shown they have an ability to reduce cancer cell proliferation as well as inhibiting tumor formation. These phytochemical can be found abundantly in cereals, cocoa, honey, fruits, nuts, olive oil, teas, vegetables, and wines. Anthrocyanins have also demonstrated a strong link to cardiovascular disease protection.Antioxidants– Molecules that prevent or delay some types of cell damage.Flavonoids– Also known as bioflavonoids, these compounds are a class of plant and fungus. In vitro studies have shown flavonoids to have anti-allergic, anti-inflammatory, antioxidant, antibacterial, anti-fungal, antiviral, and anti-cancer activity. Common foods containing flavonoids are: black tea, blueberries, citrus, cocoa, parsley, peanuts, and wine.Phenolic acids– Phenolic acids are a type of polyphenol. Other polyphenols include flavonoids. Phenolic acids have antioxidant and anti-inflammatory benefits. These polyphenols are found abundantly in plant-based foods.Quercetin– A flavonoid rich in antioxidants. Quercetin has an antihistamine effect which helps alleviate watery eyes, a runny nose, and swelling. Quercetin has also been found to support cardiovascular health.Rutin– A flavonoid that helps with vitamin C absorption and collagen production in the body. This flavonoid can help with treating hemorrhoids, high blood pressure, and reducing cholesterol levels.Additionally, elderberries contain a high level of vitamins C, A, and B6 and are also naturally high in iron, potassium and betacarotene. 2. Elderberry provides cold and flu reliefElderberries are rich in anthrocyanidins which are known to have immunostimulant effects. Stimulating and strengthening the body’s natural fighting mechanisms makes for a much more speedy recovery. When it comes to cold and flu relief, elderberry reduces swelling in the mucus membranes, helping to reduce cold and flu symptoms as well as sinusitis. A 2016 double blind placebo controlled trial of 325 people showed that using elderberry reduces the duration of a cold and its symptoms by 2 days.Other studies have shown the flavonoids present in elderberry extract to bind to the H1N1 human influenza virus. Repeat findings of elderberry extract’s ability to significantly improve most flu symptoms has led researchers to conclude that the extract is effective in controlling influenza symptoms. The extract was found to be so effective that it was compared with Amantadine and Oseltamivir (Tamiflu)— prescription medications.3. Elderberry relieves allergies Since elderberry stimulates immune function and reduces inflammation, it’s a great natural remedy for allergies. Elderberrycan help effectively relieve allergy symptoms such as inflammation of the sinuses, sneezing, swelling, itching, watery eyes, runny nose or stuffy nose. This potent herbal remedy also aids in detoxification.4. Elderberry naturally lowers blood sugar Elderberry has traditionally been used as a natural remedy for diabetes. Studies have shown elderberry extract naturally helps lower blood sugar levels in two ways, a) by stimulating the metabolism of glucose, b) stimulating the secretion of insulin.How to consume elderberryElderberry is available in a wide variety of preparations, including:AstringentCapsulesInfusionsJamsJuiceLiquidLozengesOintmentsPillsPowderSpraysSyrupTeaWineFor best results, pair elderberry with echinacea and olive leaf. |
This article is an excerpt from Atomic Habits, James Clear’s New York Times bestselling book.
My college strength and conditioning coach, Mark Watts, taught me an important lesson about how to be thankful that applies to life outside of the gym as well as inside it…
As adults, we spend a lot of time talking about all of the things that we have to do.
You have to wake up early for work. You have to make another sales call for your business. You have to work out today. You have to write an article. You have to make dinner for your family. You have to go to your son’s game.
Now, imagine changing just one word in the sentences above.
You don’t “have” to. You “get” to.
You get to wake up early for work. You get to make another sales call for your business. You get to cook dinner for your family. By simply changing one word, you shift the way you view each event. You transition from seeing these behaviors as burdens and turn them into opportunities.
The key point is that both versions of reality are true. You have to do those things, and you also get to do them. We can find evidence for whatever mind-set we choose.
I once heard a story about a man who uses a wheelchair. When asked if it was difficult being confined, he responded, “I’m not confined to my wheelchair—I am liberated by it. If it wasn’t for my wheelchair, I would be bed-bound and never able to leave my house.”1 This shift in perspective completely transformed how he lived each day.
I think it’s important to remind yourself that the things you do each day are not burdens, they are opportunities. So often, the things we view as work are actually the reward.
You don’t have to. You get to.
CHECK HIS SITE FOR MORE GOOD TIPS (the link is above)
Anthrocyanins– Anthrocyanins are a subgroup of the flavonoid class. Research has shown they have an ability to reduce cancer cell proliferation as well as inhibiting tumor formation. These phytochemical can be found abundantly in cereals, cocoa, honey, fruits, nuts, olive oil, teas, vegetables, and wines. Anthrocyanins have also demonstrated a strong link to cardiovascular disease protection.
Antioxidants– Molecules that prevent or delay some types of cell damage.
Flavonoids– Also known as bioflavonoids, these compounds are a class of plant and fungus. In vitro studies have shown flavonoids to have anti-allergic, anti-inflammatory, antioxidant, antibacterial, anti-fungal, antiviral, and anti-cancer activity. Common foods containing flavonoids are: black tea, blueberries, citrus, cocoa, parsley, peanuts, and wine.
Phenolic acids– Phenolic acids are a type of polyphenol. Other polyphenols include flavonoids. Phenolic acids have antioxidant and anti-inflammatory benefits. These polyphenols are found abundantly in plant-based foods.
Quercetin– A flavonoid rich in antioxidants. Quercetin has an antihistamine effect which helps alleviate watery eyes, a runny nose, and swelling. Quercetin has also been found to support cardiovascular health.
Rutin– A flavonoid that helps with vitamin C absorption and collagen production in the body. This flavonoid can help with treating hemorrhoids, high blood pressure, and reducing cholesterol levels.
Additionally, elderberries contain a high level of vitamins C, A, and B6 and are also naturally high in iron, potassium and betacarotene.
Elderberries are rich in anthrocyanidins which are known to have immunostimulant effects. Stimulating and strengthening the body’s natural fighting mechanisms makes for a much more speedy recovery. When it comes to cold and flu relief, elderberry reduces swelling in the mucus membranes, helping to reduce cold and flu symptoms as well as sinusitis. A 2016 double blind placebo controlled trial of 325 people showed that using elderberry reduces the duration of a cold and its symptoms by 2 days.Other studies have shown the flavonoids present in elderberry extract to bind to the H1N1 human influenza virus. Repeat findings of elderberry extract’s ability to significantly improve most flu symptoms has led researchers to conclude that the extract is effective in controlling influenza symptoms. The extract was found to be so effective that it was compared with Amantadine and Oseltamivir (Tamiflu)— prescription medications.
Since elderberry stimulates immune function and reduces inflammation, it’s a great natural remedy for allergies. Elderberrycan help effectively relieve allergy symptoms such as inflammation of the sinuses, sneezing, swelling, itching, watery eyes, runny nose or stuffy nose. This potent herbal remedy also aids in detoxification.
Elderberry has traditionally been used as a natural remedy for diabetes. Studies have shown elderberry extract naturally helps lower blood sugar levels in two ways, a) by stimulating the metabolism of glucose, b) stimulating the secretion of insulin.
Elderberry is available in a wide variety of preparations, including:
For best results, pair elderberry with echinacea and olive leaf.
Essential oils are one of the best options for restoring respiratory health. Essential oils can quickly and effectively reduce swelling in the respiratory tract, help expel phlegm, and improve breathing. Their effect can be felt almost instantaneously and there are little to no adverse side effects when using essential oils for respiratory health. There is quite a large variety of essential oils available for an even wider variety of ailments. Most essential oils are available at low price points, making them a great, inexpensive choice for addressing ailments. A little oil, just a few drops goes a long way, so even the pricer oils are still a great, natural, cost-effective option.
Lemon oil is an effective essential oil when it comes to congestion and coughs. The oil is derived from the skin of lemons. It is useful for treating sore throats in association to its antioxidant, antibacterial, and antioxidant properties. Scientific research and evidence has shown that lemon oil is able to inhibit bacteria growth and improve the immune system. In the Journal of Antimicrobial Chemotherapy, a study was published in 2001, which stated that antibacterial actions of essential lemon oil was effective against allergy and cold symptoms.
Frankincense essential oil is regarded as a highly powerful oil. Years ago, frankincense was at a stage valued higher than gold. Today, this oil is a fantastic anti-inflammatory when it comes to clearing nasal passages and lungs along with the regulation of breathing patterns. More specifically, it can assist in expelling phlegm out of the lungs. When treating a cold or a cough, use 2 to 3 drops of the oils in a diffuser.
Studies have suggested that antispasmodic activities in peppermint essential oil can help relieve coughing. This oil is better known when it comes to its antibacterial, antiviral, anti-inflammatory, antispasmodic, expectorant and antimicrobial properties. Peppermint is commonly used to treat respiratory infections, sinus infections, colds, sore throats and coughs. In the Journal of Ethnopharmacology a study which was published in 2010 has suggested antispasmodic activities in essential peppermint oil assists in relieving coughs. Menthol present in this oil is believed to soothe and calm sore throats, while relieving a cough in the way of thinning mucus.
This essential oil contains antiviral, antiseptic and antimicrobial properties. Tea tree is a fantastic oil when it comes to bronchial congestion. This oil has been discovered to exhibit exceptional protective activities against fungi, yeast, and bacteria, which can be found in a study which has was released in 2000 from a German research team. Microbes are what cause inflammation that can deplete the person’s immune system, which often results in congestion and coughs and susceptibility to other infections. Tea tree essential oils contain antiviral, antiseptic and antimicrobial properties that fight off these microbes. This essential oil is effective for bronchial congestion, coughs and sore throats. For relief, apply 15 drops of a good quality tea-tree oil to the sinuses and neck for an effective cough remedy.
Eucalyptus oil is proven to be a useful aid for treating upper-respiratory infections and congestion. This high-quality oil also loosens mucus and lowers respiratory inflammation inside the lungs. Eucalyptus is found in a variety of over-the-counter products when it comes to congestion, cough and cold relief. This is an essential oil associated with many health benefits when it comes to its effective abilities in improving respiratory circulation, stimulating the immune-system, and providing antioxidant protection. The active ingredient in this oil is known as cineole. With many long-term studies it has been indicated that essential eucalyptus oils are useful for treating upper-respiratory infections and congestion.
Research suggests that thyme essential oil can assist in supporting the respiratory and immune systems. This is a preferred essential oil when it comes to congestion and coughs in association to its antimicrobial, antioxidant and antibacterial properties. It is these effects which assist in supporting the respiratory and immune systems. In 2011, there was a study which was published in the Medicinal Chemistry journal, where researchers studied the response of thyme oil to 120 different bacteria strains which were isolated from people suffering from respiratory infections. Results showed that this oil displayed strong activities against each of these bacteria strains. This means thyme essential oil is ideal for congestion, coughs and sore throats caused from colds and flu and other related illnesses.
This essential oil features over 87 active ingredients that includes antimicrobial, antifungal, antibacterial and antioxidant agents. Juniper Berry essential oil has a sweet and woodsy smell, which is found in various aromatherapy blends, fragrance sprays, and even household-cleaning products. This is an essential oil that is typically used for treating respiratory infections as well as sore throats. Research has gone onto show that this important essential oil has over 87 active ingredients which include antimicrobial, antibacterial, antioxidant and antifungal agents. In 2003 a study appeared in the Phytotherapy Research journal which discovered that antimicrobial activities associated with juniper oil was due to the combination of the compounds known as alpha-pinene, p-Cymene and beta-pinene.
Clove essential oil displays antimicrobial activities against various multi-resistant bacteria. This essential oil is commonly used for relieving sore throats, boosting the immune-system, which has to do with its stimulating, antiviral, antifungal, anti-inflammatory, antimicrobial and antiseptic properties. In the journal Phytotherapy Research a study was published in 2007 discovered that essential clove oil displays activities against several multi-resistant bacteria. When you feel a sore throat coming on or you are starting to cough, placing 1 drop of clove oilon your tongue is an effective remedy for these common issues.
Aromatherapy is an age old yet effective practice to relieve coughs. Add drops of your chosen essential oil into the diffuser. Diffusers are one of the best ways to use the above mentioned essential oils when it comes to coughs and congestion we described earlier on. A diffuser of high-quality is a worthwhile investment.
These diffusers work on breaking the essential oil down into very small molecules that spread through the air. This process will improve air quality in the room that you use it in. In this way diffusers work well for treating flu, sinus infections, congestion and colds.
One of the other effective ways to use essential oils for colds, congestion and coughing is to add the oil into hot water in a bath. Relaxing and soaking in hot water with your favorite essential oil can work wonders when fighting a cold or flu. Below is a recipe you may want to try:
Ingredients
– 6 Drops of Tea Tree Oil
– 2 Drops of Thyme Oil
Directions
Add both the essential oils into hot or warm water in your bath. Make sure you do not use more than the recommended dose of thyme oil as it can result in irritation. You can also add some lavender or eucalyptus epsom salt to relax your muscles and joints. Relax and enjoy a healing bath.
Clearly sugar is not great for us. But it’s so delicious! And as anyone who’s ever sat down to eat one Twizzler and accidentally polished off the bag (i.e. everyone) can tell you, once you start, it can be hard to stop. If only there was something to interrupt the deadly and delicious cycle…One way people have been derailing the sugar train throughout the years is by consuming gymnema—a woody vine that grows in the tropics of India, Africa and Australia. Its bitter compounds have been used for centuries in traditions like Ayurveda to control sugar cravings and treat diabetes. There’s even evidence of the herb in use 2000 years ago in the treatment of “honey urine,” a poetic and archaic term for diabetes.
Gymnema’s most noticeable effect is that after tasting the leaf, your tongue will be temporarily unable, or less able, to taste sweetness in foods. A 2017 article in Japan’s peer-reviewed Journal of Oral Biosciences found that gymnemic acids can interact with the sweet taste receptors on your tongue, making you unable to taste sweetness. And a 2014 study in Biomed Research International found that gymnemic acids are chemically similar to sugar molecules, and can block activation of the taste buds. It’s generally a pretty effective mechanism. Human trials reported in a 1999 article in the journal Chemical Senses found people’s ability to identify sweet taste after a gymnemic acid rinse in a blind trial was reduced to only 14 percent of their natural ability to identify it. Gymnemic acids can also attach to the surface of the intestine, preventing absorption of sugar molecules and reducing blood sugar levels. MedlinePlus reports that gymnema supplements “might affect blood sugar levels,” although the available evidence is not strong. For that reason, they caution that people with diabetes watch for signs of low blood sugar, and be especially careful of taking the herb alongside insulin.
The herb and its compounds are available over the counter, in several forms. Which one you choose depends on the effects you’re hoping for, and how much you mind bitter flavors.
One of the traditional ways of taking gymnema is as a tea. But it’s a bitter brew, and not the most user friendly way to consume the herb. You can buy packaged teabags like these from Amazon (currently $6 for 18), which gets such glowing reviews as “The taste is not bad like some reviewers mentioned.” It’s inexpensive and straightforward, at least.
Gymnema is readily available in capsule or tablet form at health food stores and even at WalMart. (Prices vary, but one of the cheaper deals is $14.99 for 120 capsules.) While the capsules may bring about the effect of blocking intestinal absorption of glucose, they’re not going to have the immediate, taste-quieting effects of the tea.
There is a way to get the sweetness-deadening benefits of gymnema without having to put up with the taste of the tea: with a flavored lozenge. It’s sold commercially as Sweet Defeat, formerly known as Crave Crush. A 60-lozenge supply costs $49.99. Sweet Defeat has funded research, published in the Journal of Psychopharmacology and conducted by clinical psychologist Dr. Eric Stice and his team at the Oregon Research Institute, on the formulation of the lozenge. Stice and his research team recruited 67 adults and had them pick their favorite candy from a stash. Each one ate a single serving, and then took the lozenge or a placebo. Then, they were offered another sweet hit. The ones who’d gotten the active ingredient were 31 percent less likely to take a second candy and those that did reported “reduced candy pleasantness.”
When Sweet Defeat’s advertisements started showing up in my newsfeed (making me feel seen, and not in a good way) it was pretty much only a matter of time until I pulled the trigger and ordered a supply. I spoke with Andrea Lawson, a customer who left positive comments on Sweet Defeat’s Facebook page, and she told me what to expect:“After I take a lozenge, anything sweet tastes really, really bad,” she says. “It’s kind of like eating cereal after you’ve just brushed your teeth.” She says that the toughest part of using Sweet Defeat is, well, using it. “The hard part is grabbing a lozenge when I’m having a sugar craving, rather than grabbing the cookie that’s right in front of me,” Lawson says. “That’s the real challenge.”Sweet Defeat’s single-lozenge foil envelopes are a cheery shade of blue. Each lozenge contains a milligram of zinc and two milligrams of gymnema leaf extract, as well as some sorbitol and spirulina extract.Like Lawson, the first hurdle for me was getting started. I knew I needed to try the lozenges, but I didn’t want to. I thought I’d start my experiment maybe tomorrow, after a nice little snort of ice cream tonight.When I finally decided to start my testing, in the interest of scientific rigor I bought a bag of mini Reese’s Peanut Butter Cups and a pint of Ben & Jerry’s Oat of This World. After two of the peanut butter cups, I tried a lozenge. It tasted minty and kind of medicinal, not at all unpleasant. My tongue felt weirdly blunted.After a few minutes, I unwrapped another peanut butter cup and, full of trepidation, bit into it.It tasted pretty great. I sat there and methodically ate [redacted] more. It didn’t slow me down on the ice cream, either.I kept a supply in my work bag and tried it several more times over the next few weeks, but it never managed to yuck my yum enough to stop me. The experience of eating it and the weirdly nice taste of the lozenge served as a reminder that I was trying to be less of a swine, so to some extent it made me more mindful, I guess.I don’t know if my love for sugar is just more powerful than other peoples’, or if it’s only a lucky few for whom gymnemic acids can truly block cravings. Gymnema does seem to work for plenty of people, even if it’s not enough to keep me out of the ice cream aisle. Gymnema products can be ordered from Emerson Ecologics http://tinyurl.com/wellevate-me-nick-soloway